A surgical ecosystem where every interface inconsistency is a use-error
Human-factors research and industrial design across a six-product FDA-regulated family, from handheld devices to OR consoles to room-scale integration.
Role
Lead human-factors researcher and industrial designer across the family
Scope
Hardware, software, OR integration
Standards
IEC 62366, FDA 21 CFR 820.30
System
6-product surgical ecosystem
Arthroscopy in the operating room: imaging, resection, and fluid management coordinated across a single procedure. Image courtesy of Arthrex.
The decision in brief
Primary constraint
Regulated surgical devices where a confusing or unreliable interface is not acceptable, and the hardware and software had to behave as one system.
The decision
Move core controls from mechanical to digital for reliability, and add per-surgeon programmability without breaking blind, by-feel use.
Outcome
One loading mechanism won all three measures in a 57-participant, three-region study and set the fluid-management direction. The footswitch speed behavior came from measured activation zones, not an assumed curve.
Role: led UX and human factors across a six-product surgical ecosystem, hardware and software. Evidence of designing the physical and the digital together under regulated constraints, a capability that transfers to any product that spans the two.
The problem
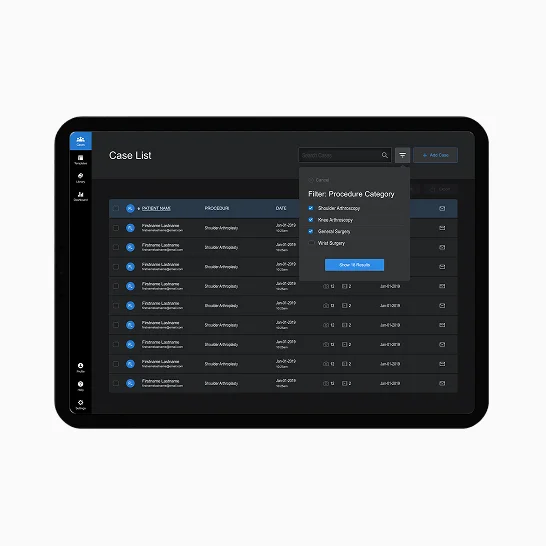
I framed the OR as a systems problem, not an interface problem.
Arthrex’s surgical product family had grown across decades, with each device designed independently. Arthroscopic procedures required clinicians to coordinate imaging, resection, fluid management, routing, and documentation across products that did not share control logic. That fragmentation created unnecessary setup effort, inconsistent behavior, and higher cognitive load during already demanding tasks. The next generation had to deliver modern capability while reducing cognitive load and meeting FDA and IEC 62366 use-error requirements.
Surgeons and OR staff worked with products designed by separate teams over decades, with inconsistencies that added cognitive load mid-procedure. The next generation needed shared physical controls, interface structure, and feedback behavior across handheld devices, console UI, room-scale integration, and post-operative communication.
Anthropometric data shaped control size, placement, and physical interaction before form.
Surgeons and circulating staff use these instruments under glove, single-handed, and often without looking at their hands. Anthropometry, ergonomic study models, and percentile-based testing produced concrete design-driving values for grip, reach, and force before any decisions were made about appearance or manufacturable geometry.
Dimension
5th %ile F
50th %ile
50th %ile
Design driver
Hand length
163
184
206
Overall hand envelope
Palm length
163
184
206
Overall hand envelope
Hand breadth at metacarpals
163
184
206
Overall hand envelope
Index finger length
163
184
206
Overall hand envelope
Thumb breadth
163
184
206
Overall hand envelope
Grip diameter, max
163
184
206
Overall hand envelope
5th to 95th percentile fit · grip, reach, force constraints · error prevention by design · Role: led human-factors research and industrial design.
Fig. 02a
Percentile-based hand measurement mapped to control geometry.
Fig. 02b
Ergonomic study models tested for grip and reach across the range.
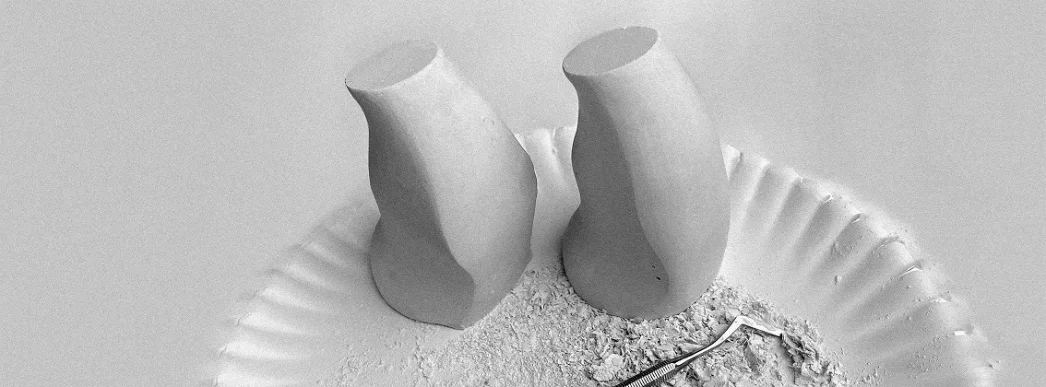
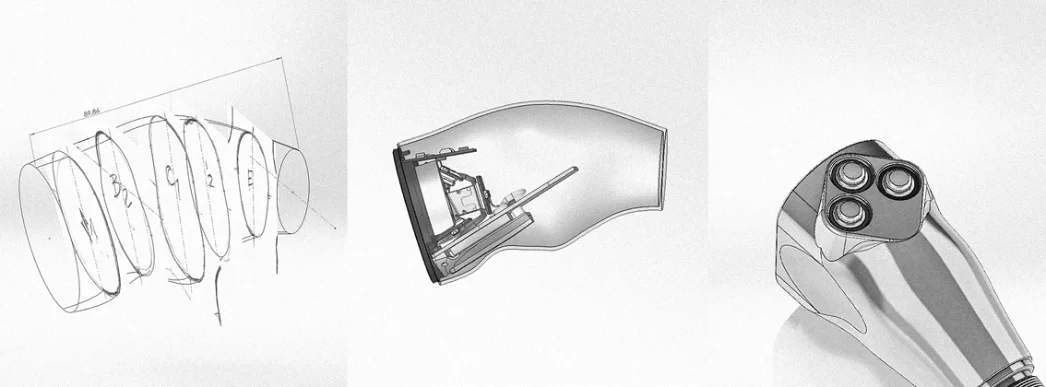
Industrial design
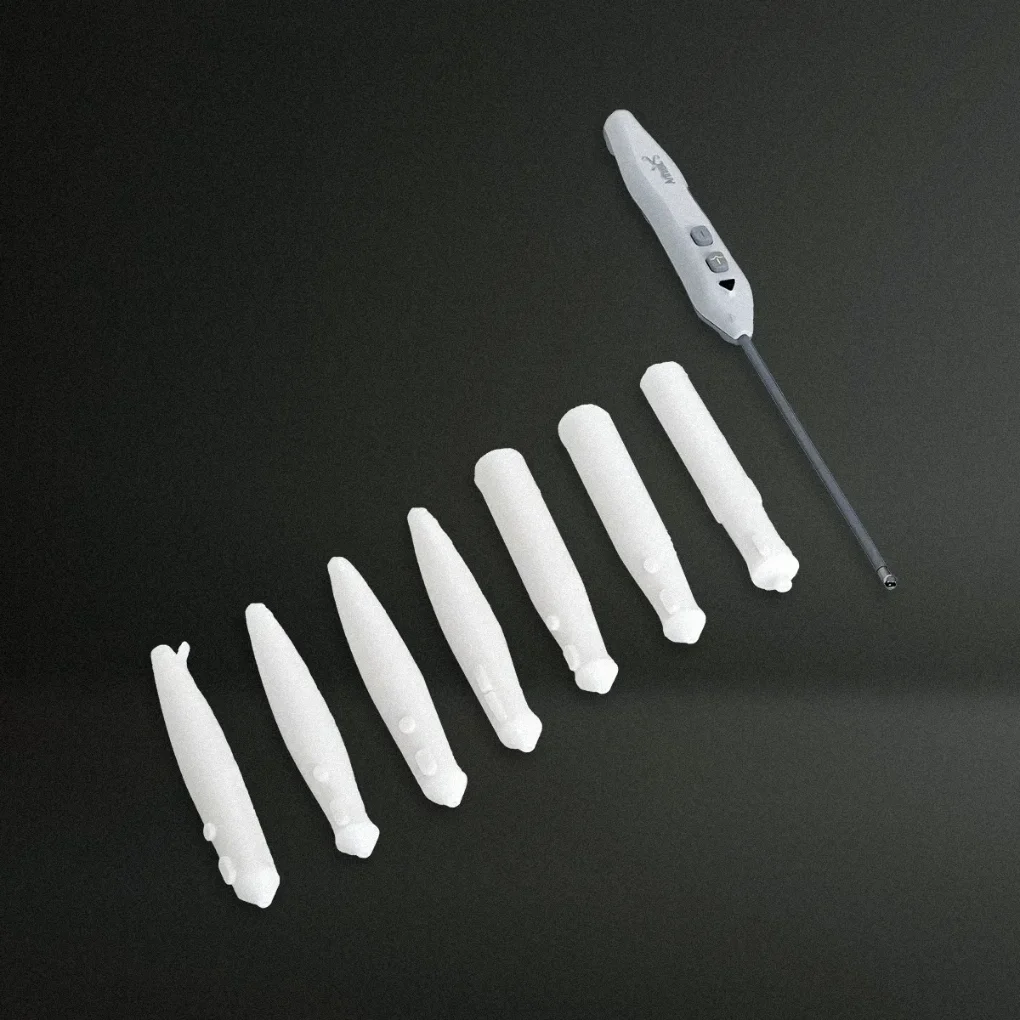
Refining the camera head for stable handling and intuitive control under gloved use.
Surgeons performing arthroscopy and endoscopy needed a camera head that felt reliable and balanced under gloved use, across the full anthropometric range, in both hands. Iterative study models, CAD refinement, and real-use testing shaped a form that supported natural hand positioning and more predictable control during procedures.
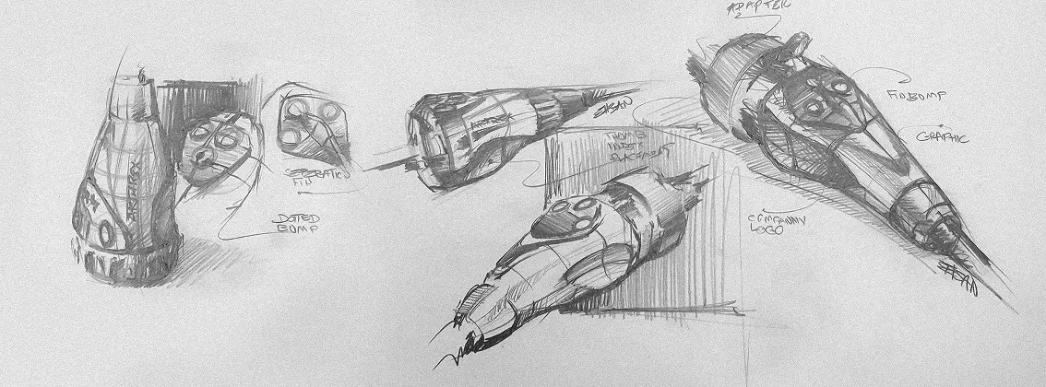
Fig. 03a
01 · Concepts explored
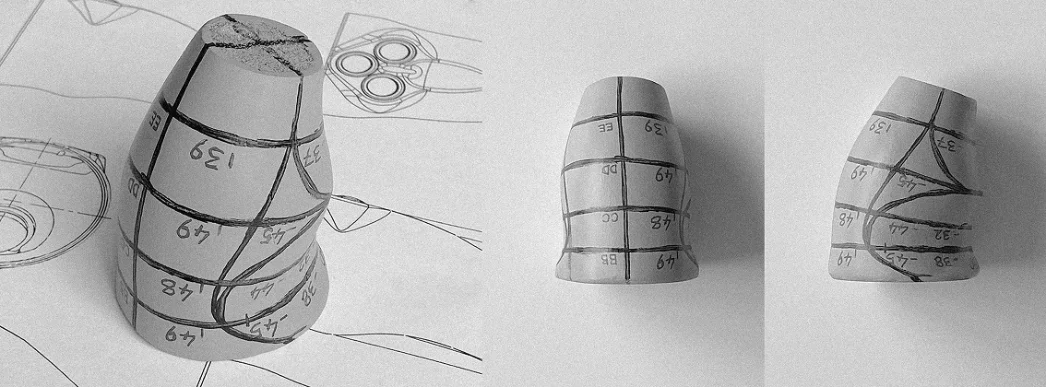
Fig. 03b
02 · Ergonomic study models
Fig. 03e
Percentile-based hand measurement mapped to control geometry.
Fig. 02b
Ergonomic study models tested for grip and reach across the range.
Fig. 02a
05 · 3D scanning to CAD
Fig. 03f
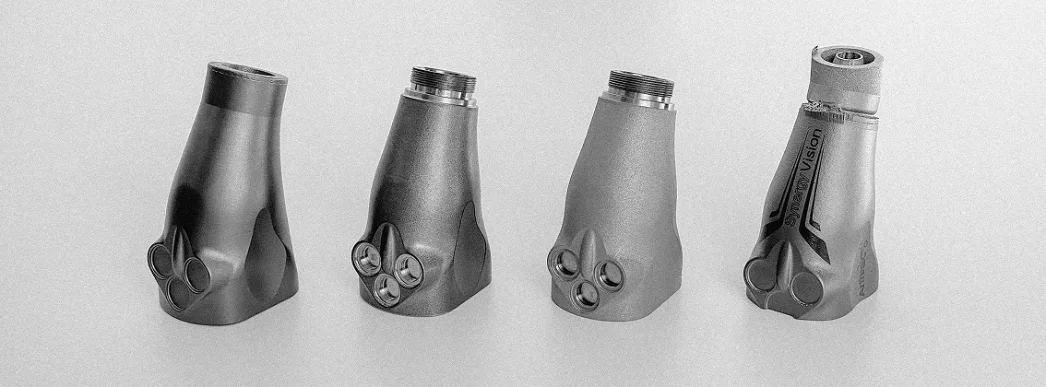
06 · Prototypes refined and tested
Final camera head: ambidextrous form with control placement set by the anthropometric range.
Formative evaluation
Testing the button form before committing to it.
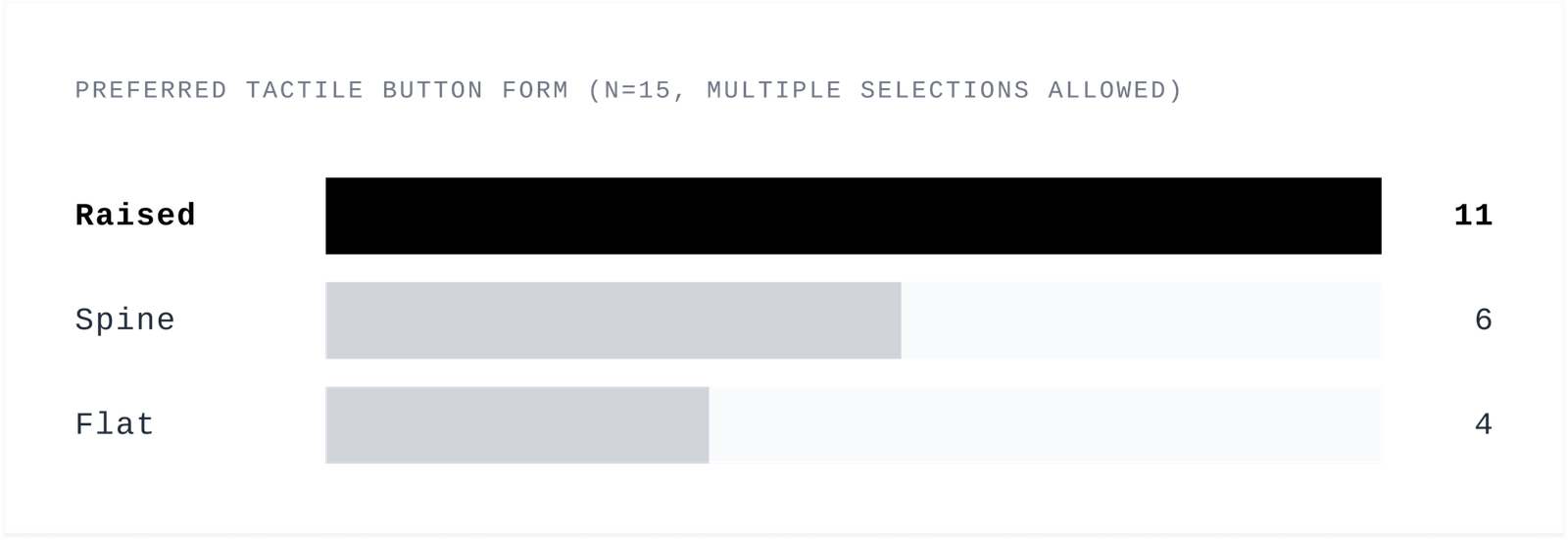
The new camera head adds a third button. It is programmable, so a surgeon can map it to their own profile and reach for it without looking, while their eyes stay on the OR screen. That customization is a real gain, but it changes the physical problem. The previous generation had two controls to find by feel. This one has three, and a wrong press during a procedure is not a small thing. The button form had to make all three reliably identifiable by touch alone.
Before committing to a direction, we ran a formative evaluation with 15 clinicians, 5 surgeons and 10 OR physician assistants. Each handled prototypes and judged how well three tactile button forms, raised, flat, and spine, supported finding the right control by feel. The raised form was the clear preference, and 11 of the 15 chose the new button design over the current generation. That result set the direction for the production form.
Fig. 03g
Across 15 clinicians, the raised form led the three tactile options and set the production direction.
11 / 15
clinicians preferred the new button design over the current generation in formative testing.